In my anecdotal estimation, the RVU compensation model is the most common model for physicians across the U.S. at least. When I was looking for my first job, most contracts came with an RVU compensation model.
But, to be honest, I didn't really understand the model all that well until even recently. And, also being honest (why is this even a phrase?..), I am not currently using an RVU compensation model. However, it is still really important for me to understand and know how to interpret/analyze RVUs. As it is for all doctors regardless of current compensation model.
So that is what we are going to be discussing here!
What is an RVU?
There's no better place to start than the beginning. Put very simply, an RVU is an abbreviation for Relative Value Unit. And a Relative Value Unit is a numerical measure of value provided via some service, treatment, procedure, or other healthcare related thing.
That's it.
Some group of people decided on what they determined the baseline value of 1 RVU to be. And then they decided how many RVUs valued each healthcare related good/service.
Therefore, RVUs are a replacement of the numerical and monetary value of a healthcare service (think office visit, procedure, surgery, etc…)
But not all RVUs are equal
Because of course not. Why keep it simple?
First, there are “facility” RVUs and “non-facility” RVUs. Just throw facility RVUs right out the window. They are not for you. They are for the hospital/center/surgery center that you perform said healthcare service at or in.
Ok, but non-facility RVUs are all for the docs right?
Nope!
Within the non-facility RVUs, work RVUs (wRVUs) represent the “work” done by a particular physician in providing this service, treatment, procedure, or other healthcare related thing.
There are other RVUs like “practice expense” (PE) RVUs and malpractice RVUs as well.
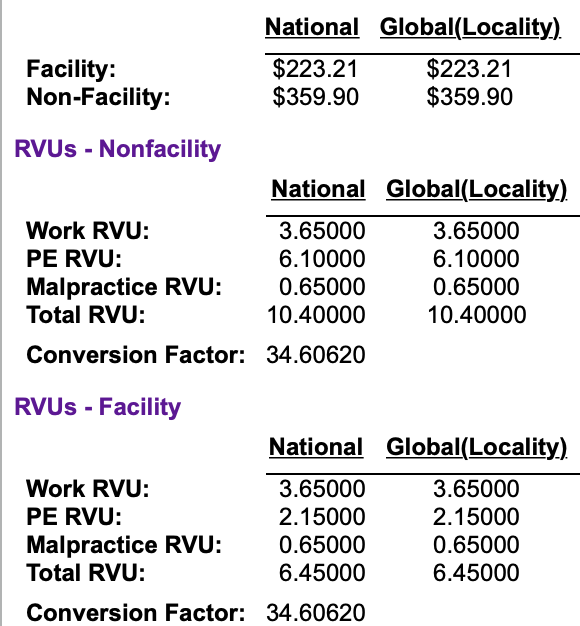
So, the non-facility wRVUs that traditionally apply to physician compensation are just a portion of the entire “RVU pie” that comes from a patient’s treatment or procedure.
Is this right or fair? Depends who you ask. But since you are asking me…no. No, it is not. However, that is how it is.
But really…
An RVU (I will now be using RVU synonymously with non-facility wRVU) is just a conversion factor. It helps to convert your work into money.
And this is the equation:
RVU * $/RVU = Your Compensation for any given medical service
For example, the average $/RVU for plastic surgeons is around $65/RVU. So, if a plastic surgeon performs a widgetplasty (not a real surgery) valued at 20 wRVUs, their compensation for that service will be:
20 RVU * $65/RVU = $1,300
And the rest of the RVU pie is similarly sliced and divvied up.
Evaluating the RVU compensation model
So, we can see that overall, the RVU compensation model is fairly simple and straightforward.
But is it good?
Well, let's compare it to the other most prominent compensation model, a pure profit and loss (P&L) compensation model.
In a P&L model, your compensation is exactly equal to how much money you bring in through your practice minus your expenses to the practice.
Advantages of the RVU system
- Easy to understand and track
- All that you need to do is figure out the RVU values of the services you provide and your $/RVU conversion factor
- Good for when patients don’t have great insurance (or any)
- The RVU model doesn't depend on money actually coming in from insurance (or anywhere else)
- You are created for the RVU just by providing the service
- Good for when your practice does not have favorable rates for certain procedures with insurance companies
- Again, you make the RVUs from performing the procedure
- And you are paid based on your $/RVU conversion factor
- Those are the only factors that matter for your compensation
- Clear division of labor among partners who work together (surgeon, co-surgeon)
- This happens a lot in surgery in particular
- Me and my partners often operate together with one being the primary surgeon and the other being the “co-surgeon”
- When this is done with an RVU model, each surgeon receives 62.5% of the allowable amount (rather than both getting 100%)
- This is easier to track than divvying up cash.
But there are disadvantages…
Disadvantages of the RVU model
- RVU values are set by CMS
- But these values may or may not be adopted by private insurance companies & your practice depending on negotiations
- This means you could be paid for less RVUs than your practice actually gets paid
- $/RVU conversion factor is also set by CMS
- But again, this may not correlate well with how much your practice is actually getting paid or pays you for your work
- For instance, one contract offer of mine would only pay me $35/RVU rather than the average $65/RVU for plastic surgeons
- Traditionally horrible for cash-based services
- For example, let's take aesthetic surgery; employees in an RVU model performing aesthetic surgery as an employee will typically make much less than colleagues in private practice accepting put of pocket cash payments
- This extends to many other medical services
- As a doctor, you only are compensated for non-facility wRVUs
- But didn’t you bring the patient to the practice/clinic/surgery center/hospital and contribute to the overall facility RVUs being paid to them?
- That doesn't seem fair
Now that we have looked at the advantages and disadvantages of the RVU compensation model, let's examine how we can address the disadvantages…
Addressing the disadvantages of an RVU model
Let's look at the main disadvantages again:
- Procedural RVU values set by CMS
- $/RVU conversion factor set by CMS
- Traditionally horrible for cash-based medical services
- You are only compensated for non-facility wRVUs
lThere is really only one way to address all of these disadvantages. Unfortunately it is something that we as physicians receive little to no training in. And we have not always done it very well. But we can learn to do it better and be very successful at it.
The answer is to negotiate!
- If you are employed, negotiate set RVU values and $/RVU conversions with your practice or employer
- If you own your practice, negotiate RVU values and conversions with private insurance companies
- Negotiate cash-based medical service RVU values with your employer
- Negotiate additional compensation based on facility and non-work RVUs
You can find more on exact negotiation strategies and other contract related topics here.
Now, let's quickly shift gears to discuss how you will typically see RVUs appear in your first (and subsequent) contracts…
How will you typically see RVUs in your first contract?
Generally, first contracts come with:
- A base salary for the first year followed by,
- A base salary with RVU bonus above a certain RVU level (Example: you keep 30% of RVUs collected above 40,000 at a conversion factor of $50/RVU) followed by,
- A pure RVU structure after the third year (Example: you make $60/RVU generated)
And as an important note, this is common in all practice environments!
This includes hospital-based and academic jobs for sure. But also private practice jobs if you are an employee of the practice.
And with all of this said, you need to make sure that you know how to negotiate your compensation if it is with an RVU model…
Before agreeing to an RVU model for compensation…
Make sure you know and understand:
- The negotiated RVU values for your most common medical services
- The exact $/RVU conversion factor you will be using
- How many RVUs the least busy person in the practice does annually
- How many RVUs the busiest person in the practice does annually
- And how many RVUs the last hire did in their first 3 years
Hesitancy or refusal to share any of this information is a big red flag!
Now let's take a look at my specific circumstances in relation to RVUs.
RVUs and Me
An RVU model made sense for my practice for a few reasons:
- I work for a public academic hospital and treat patients across the SES/insurance spectrum
- I do a lot of microsurgery with my partners as co-surgeons
- Aesthetic surgery is only ~10-15% of my practice
But…I ended up choosing a non-RVU compensation model. Why?!
Well, it really was for behavioral rather than practice or compensation-based reasons. I know myself well and I am the type-A person who will chase a carrot off of a cliff.
I never wanted to feel like I was “RVU chasing.” So, I instead negotiant a flat, non-RVU based salary that I felt was very fair.
However I still use RVUs in my compensation negotiations
I track all of my procedures, their associated total and wRVUs, and the average $/RVU conversion factor.
Therefore, when I re-negotiate my compensation, I use this data to drive my new salary!
In the end, why does all this matter?
It matters for at least a few big reasons.
For one, the equation to build wealth and achieve financial freedom is simple. You just need to increase and invest the margin between what you make and what your spend. And clinical compensation is the major contributor to “what you make” for most physicians.
For two, you really need to know your value as a doctor. And understanding RVUs helps you to do that. Here are 4 helpful methods to defining your value as a physician…
And lastly, feeling like you receive fair compensation plays a big role in your clinical fulfillment, satisfaction, and freedom from burnout. This was big for me. It makes sense to understand compensation models and give this proper consideration in your practice!
But remember, you can diversify with alternative streams of income to supplement or even replace your clinical income! Here are some resources…
- Physician Side Gigs to Make You Passive Money
- 7 Ways to Get Started with Physician Consulting
- 3 Easy Ways Doctors Can Convert Earned Income into Passive Income
What do you think? Do you agree with the RVU model? How would you change it? How does your compensation work? Let us know in the comments below!












5 Responses
I am recently retired from a privately owned group practice of primary care Internists and Pediatricians. About 10 years ago the providers in the Adult Medicine group suspected that the way our Partnership was distributing the businesses profits, our “salary reconciliations,” was favoring the Pediatricians. The formula had been based on the unadjusted percentage of the total non-facility wRVUs each partner billed. When we compared the partners salaries to the regional and national salary data for similar providers we determined that our Adult providers were correct, compared to their regional and national peers they were being underpaid and conversely the Pediatric partners were receiving higher salaries than their regional and national peers. We only did a three year look-back so we don’t know how long our dependence on the CME model caused a systemic problem with our salary structure. This inquiry led to considerable discussion about how to devise a more equitable plan; eventually we came up with one. The moral of my story is that it’s important to look at the consequence of using CME’s as the guide for determining value of your work. If a CME based formula doesn’t lead to what look like reasonable salaries for multiple providers over multiple years, then it isn’t a good formula. And, even if it looks like a good formula someone, who “has no skin in the game” needs to be keep an eye on how its is performing. over time.
Very interesting. And I agree that we always need to look at this closely. Question though – were the pediatricians producing more wRVUs than their adult counterparts?
This is the kind of thinking that is used to make sure that pediatricians continue to be underpaid. It is a self-fulfilling prophecy. They tell you that you are making more than the average pediatrician so find a way to lower your salary. Then your salary goes back into the denominator of all the other underpaid doctors to keep the average low.
Let’s look at this differently: Say the FM docs in the group are given a conversion factor of $45/RVU and the pediatricians get $40. Now they both see a child for a well visit. If that has an RVU value of 1.0, one physician gets paid $5 more for doing the same thing with less training in that area of medicine. Multiply that by hundreds-thousands of patients yearly, and you can see the effect. This doesn’t even account for the fact that younger kids are “worth less” than the older ones. Nevermind the daily phone calls from frantic parents and free advice they get at this age (that’s a whole different issue).
In my situation this didn’t even factor in that the family docs were paid extra to supervise NPs. When they had a question about a kid though, who do you think they asked? As much as I would want to tell them to ask their supervising physician, no pediatrician worth their salt can say no to helping a kid. As much as I valued many things about being in a multispecialty group, I could never join one again due to the constant feeling of being undervalued.
Tho you addressed the massive oversight later, your initial “throw out the facility RVU” is a terrible approach! It’s that facility RVU that drives so many of the deals that have docs working for “the hospital” and the patients getting gouged for e fee that didn’t exist before the hospital bought your group, thus enabling so many pencil pushers to have fat salaries on your back. When negotiating, those numbers must be on the table; and you didn’t point out that to the latest of my knowledge, when there is a facility fee on a given “event” the work RVU is lowered!
I 100% agree that facility RVUs should be considered when negotiating although most administrators will push back on it, it is important to stand firm!