One of the biggest misconceptions doctors carry is the one I carried early in my career. I assumed specialty choice determined my earning potential.
We all heard it in training.
“Ortho makes the most.”
“Neurosurgery clears the top.”
“Plastic surgery pays well.”
Those ideas are directionally true if you only look at averages. But after practicing, starting my own practice, and talking with thousands of physicians through PPS, I realized something far more important.
The biggest pay gap in medicine is not between specialties. It is inside them.
Two doctors with the same board certification can be separated by hundreds of thousands of dollars a year. Over a career, the difference easily reaches seven figures.
To explore why, I teamed up with Dr. Rob Anderson. Rob is a practicing anesthesiologist and the co-founder of Marit Health. Marit already has one of the largest anonymized datasets of physician compensation, and they recently made it even better by giving verified clinicians a MGMA snapshot for their own specialty after they share their anonymous salary. I added my own experience across plastic surgery, private practice, and physician finance.
Here is what the data shows.
The Pay Gap Range Inside Each Specialty is Enourmous
Residents and fellows often choose jobs based on the average income for their specialty. The problem is that averages smooth out all the real differences that matter.
Two physicians in the same specialty and even the same city can live in completely different financial worlds depending on how their job is structured.
One surgeon is employed on a salary with a small bonus. Another is a partner who operates at higher volume with access to ASC distributions.
Same specialty. Very different outcome.
This happens outside procedural fields too. A hospitalist who takes night shifts or ICU blocks or negotiates a productivity bonus can earn much more than a colleague who works a flat schedule.
Across the Marit data, the top 10 percent of physicians earn between one and a half and three and a half times more than the bottom 10 percent. The exact multiplier depends on the specialty.
Spread that difference over a thirty year career and you can see exactly how some physicians retire at 45 while others need to work into their sixties.
I see the same thing in plastic surgery. I know people who trained at the same programs I did. We graduated the same year. Within five years, our incomes were half a million dollars apart. The difference was not effort or talent. It was job structure.
You can explore real compensation distributions for your specialty on the Marit platform.

• Marit has one of the largest anonymized datasets of real physician compensation.
• Verified physicians get a customized MGMA snapshot for their specialty.
• All you do is share your anonymous salary to unlock it.
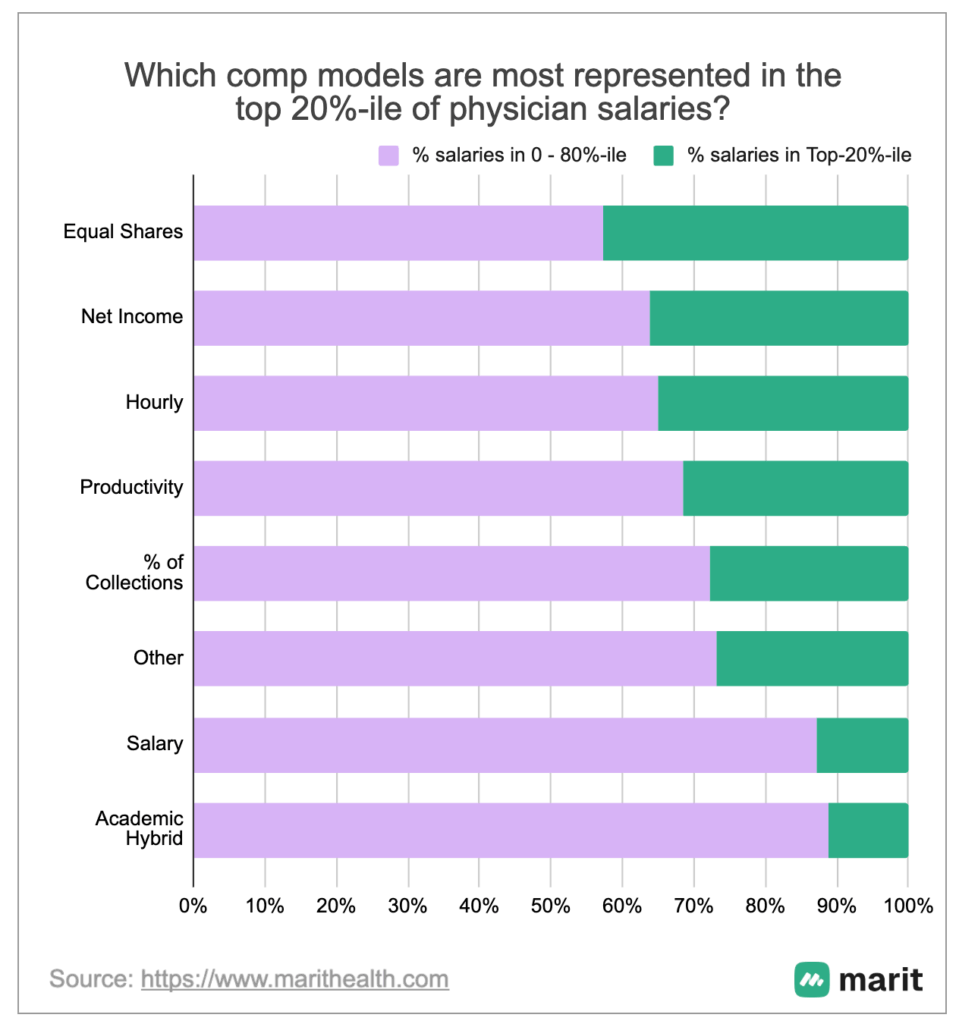
What the Top Earners Do Differently
After reviewing thousands of real salary submissions, two clear patterns show up among the highest earners in every specialty.
Ownership and Alignment Matter More Than Anything Else
Physicians who are self-employed or who have:
• a partnership track
• a collections or productivity model
• ASC or ancillary equity
• transparent equal share models
Consistently appear in the top income brackets.
You can even see it in their tax documents. K-1 income shows up far more often among high earners than pure W-2 income.
When you participate in the economics of the practice, your ceiling rises. That is true across almost every specialty.
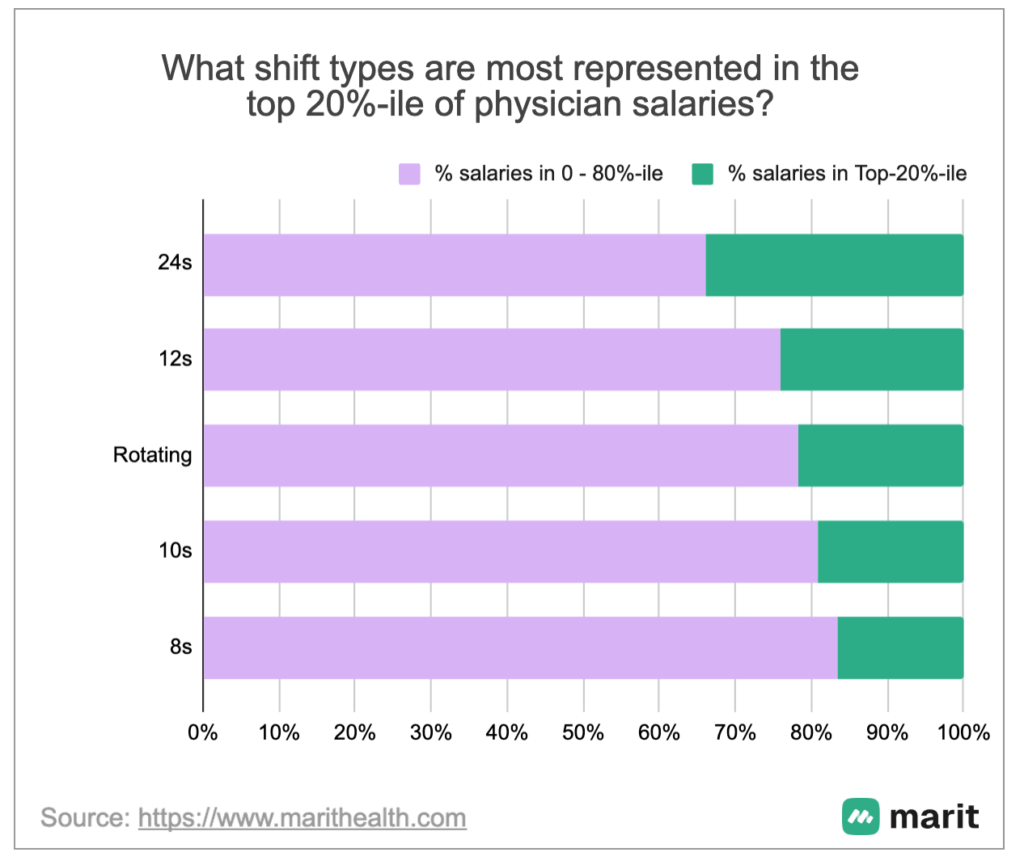
Hours and Schedule Can Increase Income, but They Are Not a Long Term Plan
The second driver of higher compensation is schedule. More calls. More nights. More weekends. Longer shifts. All of this will move you up the income range in many specialties.
But these levers come with real costs. The lifestyle and health tradeoffs compound over time. They might help for a season, but they cannot carry your whole career.
This is why I chose to be paid via a salary, rather than chase RVUs or more call/cases. Too many physicians think the solution to feeling behind financially was to work more. More cases. More hours. More call.
That approach only adds stress and pulls time away from everything else.
My progress started when I moved in a different way. I used my free time to learn how money works. I used that time to negotiate my salary using data. I built my financial plan. I started The Prudent Plastic Surgeon. I built multiple income streams.
Working more can raise income for a while. It will not give you the freedom, stability, or ceiling that a well structured career can.
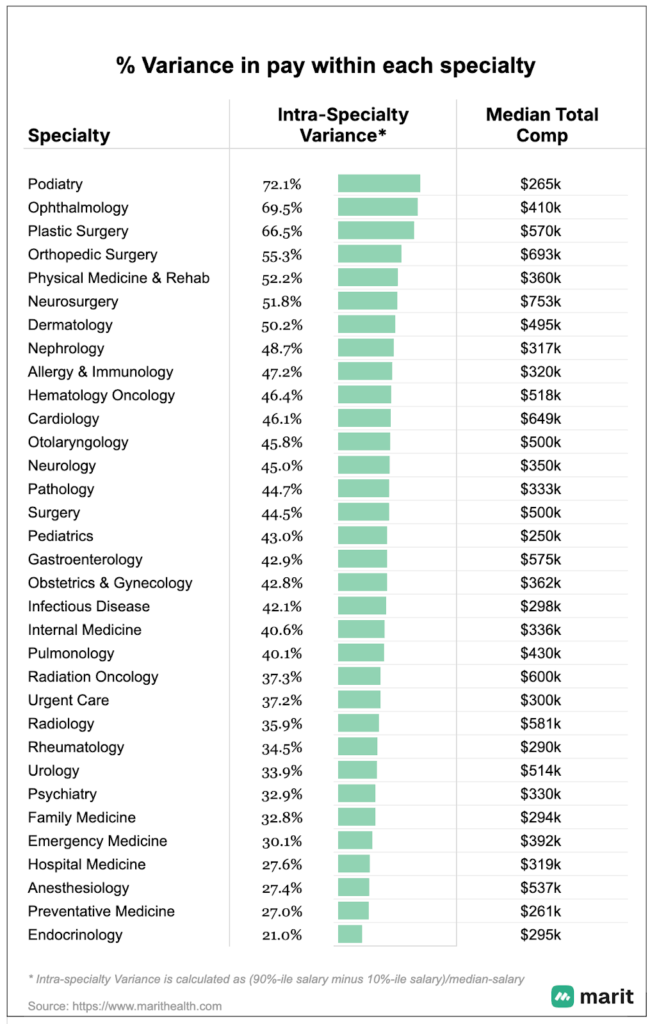
Which Specialties Have the Widest Pay Spread
The most useful insight from the Marit dataset is not which specialties earn the most. It is which specialties have the widest income range. That range determines how much control you have over your compensation.
High Variance Specialties
These specialties show the largest differences between the 10th and 90th percentile:
• Plastic Surgery
• Orthopedic Surgery
• Ophthalmology
• Neurosurgery
• PM and R
• Podiatry
The reason is simple. Structure plays a huge role.
Your income depends on things like:
• ownership or ASC equity
• OR time
• procedural volume
• payer mix
• access to ancillary revenue
This is why two plastic surgeons with identical training can end up half a million dollars apart within a few years. The difference is not clinical skill. It is the financial structure around their work.
Medium Variance Specialties
These specialties offer meaningful upside but with more standardized compensation:
• Dermatology
• Cardiology
• Gastroenterology
• ENT
• Hem and Onc
Many of these fields use blended models that mix salary, productivity, and some equity.
Low Variance Specialties
These specialties have the tightest income bands:
• Hospital Medicine
• Emergency Medicine
• Radiology
• Preventive Medicine
Compensation is tied to shifts and staffing ratios. There is stability, but less room for income growth from structure.
Conclusion:
Your specialty’s income variance tells you how much control you have over your compensation.
High variance specialties reward intentional structure.
Low variance specialties reward schedule decisions.
Medium variance specialties sit in between.
What matters most is choosing a job structure that fits your goals. The average salary you saw online will never tell you that story. The full income distribution will.












9 Responses
Lots of variables involved. Cosmetic surgery vs reconstructive. Urban vs rural practice.
Absolutely!
how do your suggestions apply to a salaried neurologist? I earn $350 K per year as a salaried cognitive neurologist, the epileptologist earns $750-800 K per year because of procedures and EEGs etc. In an hour I make 3 and some change wRVUs for a new consultation and they read 12-15 EEGs and make about 12-15 RVUs in the same time. There is no way a nonprocedural subspecialty can compare with a subspecialty with several procedures. The game is rigged at the top.
I totally get your frustration. My thought would be that, in your case, it is not necessarily a different practice activity but rather a different practice setting that could unlock a much higher income
The game isn’t rigged it’s very transparent and has been for decades. Go do a fellowship in epilepsy or Pain management. It costs 350k in list income which you can make back in a year.
As an anesthesiologist I’m still working at age 75. At $250/hr 2-4 days a week. My first year out of residency I was paid $60,000 yearly, a standard amount back then. Gradually my salary increased to $95,000 then $140,000 then $245,000 and ultimately to $310,000 and that was with taking call. My IRA contributions were limited to $2250 per annum total for me & my stay-at-home wife. I paid for my 3 children’s college tuitions. I still don’t have $500,000, let alone $1,000,000 in my savings. Therefore I still work. And with the nationwide doctor shortage I’d feel guilty retiring anyway.
Would you do anything different if you could go back?
I’m not sure its fair to say, “Those ideas are directionally true if you only look at averages.” The point is that you can always make less, that’s easy. So comparing the lower end of the pay scales has no meaning. But you can’t always make more; each speciality has its ceiling, and the ceiling is where the real wealth disparities occur.
This is true. The real question is how to get to that top end…