Let’s start with the part no one wants to say out loud: physician pay is under siege and on the decline.
For the longest time, I have been a huge advocate for physicians more openly sharing their salary. To withhold it only puts us all at a disadvantage. Those that we negotiate pay have more data and know more about physician pay. And we go in with our eyes closed. Being tight-lipped only diminishes our power to negotiate.
And until recently, this was a grass roots effort. By working to define our value better, doctors could gain more leverage and attain more fairly aligned compensation like I did with my last contract negotiations.
However, an important new tool has emerged!
Rob Anderson, MD, a practicing Anesthesiologist at NAPA (North American Partners in Anesthesiology) in Richmond, Virginia co-founded Marit Health, a Pay Transparency Platform for Medicine. Marit is a free, community-powered anonymous salary solution for physicians and APPs. I recently just signed up and contributed my data.
And I've asked Rob to share more about the physician pay decline trend and how pay transparency via Marit can help all physicians.
The concerning physician pay decline trend
Despite inflation, rising complexity of care, and growing administrative burden, physicians have seen steady cuts to their professional fees. Meanwhile, facility fees, the portion of healthcare dollars that go to hospitals and health systems, continue to climb. The people delivering care seem to be constantly falling behind.
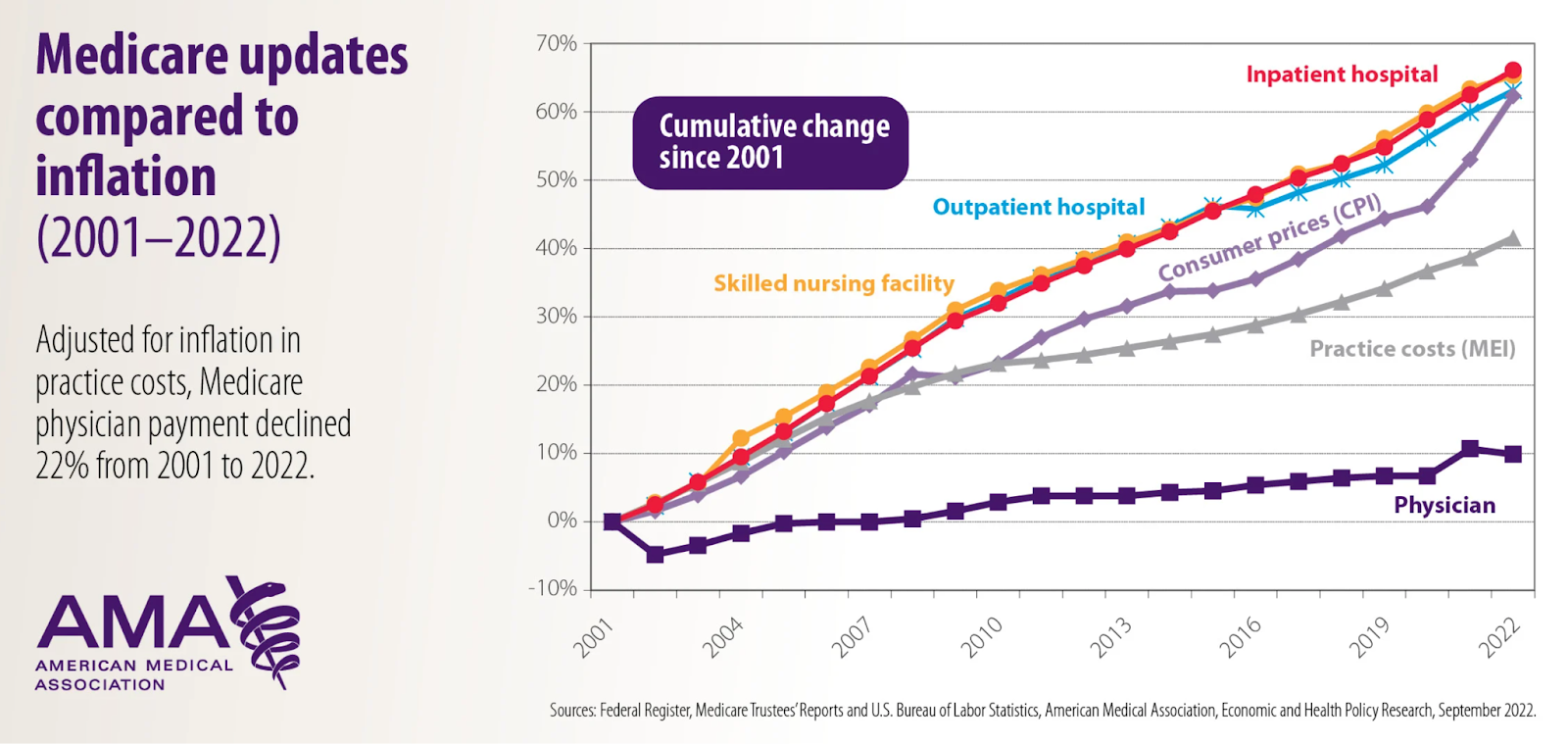
This isn’t just belt-tightening. It’s a decades-long erosion of physician compensation, with no clear end in sight.
Why don’t we just unionize?
When the topic of fair pay and physician pay decline comes up, the reflexive answer by some is: Organize. Form a union!
That sounds appealing in theory, but the reality is complicated. Most physicians work in fragmented settings, across hundreds of private practices, health systems, and contract types. Many are bound by restrictive covenants or work in states with legal barriers to physician unionization.
While unionizing can be effective in some situations, it is a significant structural change and not an easy near-term fix. Even in places where unions exist, results are mixed. It’s a tool, not a silver bullet. So, if we want to do something NOW – without legislation or third parties – what’s the solution?
The case for salary transparency
Let’s be honest: when it’s time to negotiate an offer, we all ask around. What are others making? What’s the going rate in our specialty? The more data you have, the better you can advocate for yourself. But too often, that information is displayed in vaguely defined medians and behind paywalls we cannot access.
We already know from other industries that transparency leads to better pay. And fairer pay. This isn’t a new idea. It isn’t radical. It’s a proven concept. And it doesn’t require legislation or permission.
If we simply choose to share what we’re paid, along with all the context around it, anonymously, securely, and safely, we can begin to change the power dynamics around physician compensation. We can negotiate with confidence. We can hold others accountable. And we can redefine fair market value based on real data, not a number set by someone else.
This isn’t a theory. I’ve seen it work.
I know this because my brother was part of the early team at Glassdoor, and I watched them as a small startup crack open the black box of employee pay and employer reviews. Suddenly, anyone could see what others earned. And just like that, negotiation became advocacy, and transparency became power.
So we built the version medicine deserves
I started testing this idea with a simple Google sheet and an anonymous salary survey for anesthesiologists and CRNAs (the specialty I know best). And just within 36 hours, more than 450 clinicians had contributed. The submissions were detailed and honest, and it was clear that there was a real appetite for something more open and accessible.
What made this even better was the depth of the information. It had not just the salary components, but all the other details that matter – tax structure, hours worked, call schedule, practice type and setting, wRVUs and collections rates, location, benefits, and more.
Since then, more than 9,000 clinicians have contributed to Marit, making it one of the largest and richest compensation data sets of its kind in medicine. Best of all, it’s fully accessible to verified clinicians and will always be free to use.
Is the data any good?
It turns out – Yes!
This is by clinicians, for clinicians, so we all want it to be accurate so we can use it for ourselves. We compared our data to well-known benchmarks – MGMA, Doximity, surveys done by the professional associations, and other publicly available datasets.
You can see that across all specialties – the numbers converge surprisingly well. But there are a few differences – the community data is more current, (e.g., MGMA is still reporting numbers from 2023), more representative (W-2, 1099, locums, large and small employers), more holistic (includes W-2 income + partnership income, etc.), so our numbers tend to be a bit higher and more accurate estimates, than what other benchmarks represent.

The power of individual compensation reports
When people think about physician compensation data, they often think about medians and averages. This is helpful, but incomplete. Compensation varies so widely by the choices we make – hours, call schedule, practice type, ownership structure, payer mix, location, etc. With the community data, we can now see all the anonymized individual data points and understand the full context. The details are all right there – every line of data is visible, anonymized, and filterable by specialty, location, setting, and more.
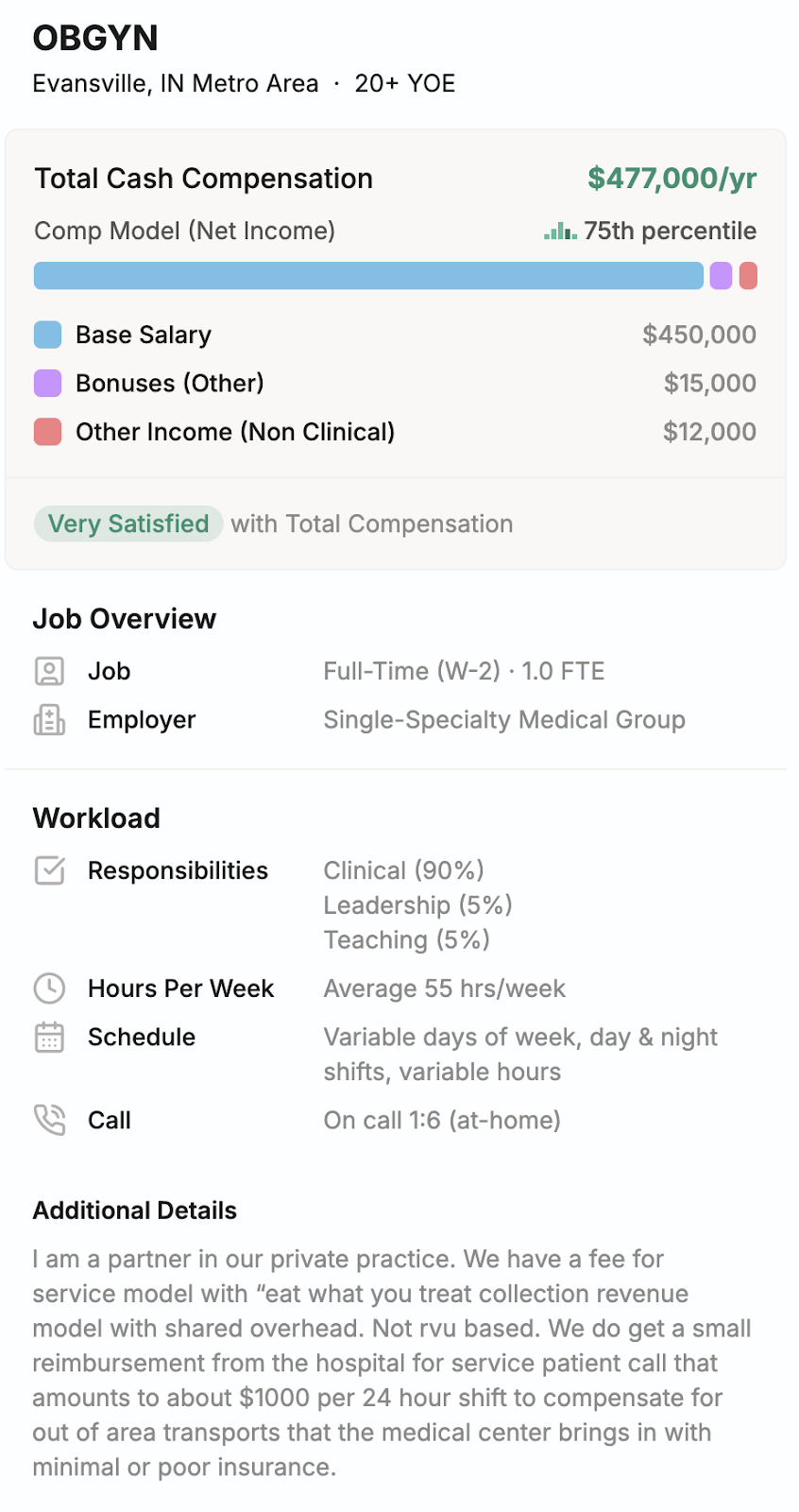
For example, this OBGYN salary in Indiana is in the 75th percentile, but they work 55 hrs/wk and are a partner in a private practice. They are 1.0 FTE, of which 90% is clinical responsibilities. These are the kinds of tradeoffs we need to understand to decide what our individual FMV is. Each of us has different priorities, and all this detailed data helps. It is not about comparing ourselves, but about learning what’s possible.
A small, collective step toward fair pay and and end to physician pay decline
Obviously, declining physician compensation is a longstanding issue, and no one effort will solve the complex, systemic issues behind it.
But sometimes, real change starts small and quietly, not by disrupting the system, but simply with people sharing what they know for the benefit of others. And as more people participate, it will only get bigger and stronger from here, moving us toward a future where physician compensation is more fair and transparent.
We cannot wait for regulators to act.
This change must be driven by clinicians, for clinicians. We’ve been silent for too long already.
Here are some actionable steps you can take to increase your compensation and help other physicians do the same:
- Learn how to define your value as a doctor
- Discover ways to increase your clinical compensation
- Explore lucrative physician side gigs
- Anonymously contribute your salary data to Marit
What do you think? Does the physician pay decline concern you? What solutions do you see? Would salary transparency help? Why or why not? Let me know in the comments below!












18 Responses
This is OUTSTANDING! Thank you!
I understand the basis for this idea but I don’t know how powerful it truly is if we are saying that salaries are going down. Don’t these numbers represent the underpayment of physicians? In many ways, it’s a self defeating number. As a FM doc, my salary is 100-150 higher than the numbers listed. My salary— nothing else. So why are we trying to label a docs/ specialty’s worth with low numbers? So they can continue to pay us less? Heck, why are we saying that the folks who take care of all patients medical problems, and not a specific part, should be the lowest compensated? Please hear me I love specialists and they are needed for my complex cases but there is a reason that everyone needs a PCP. That is what makes me valuable. Just like a specialist is compensated for the value they input. I think there are a lot of bias and unfair nuances that this type of reporting in our business reinforces. If we really want fairness in payment, it needs to be to all specialities. Not just a fêted few.
Ps. Everyone states there is a crisis in primary care and it doesn’t take a genius to figure out why. It’s time that the government, insurance companies and big business are required to “put their money where their mouth is”. It seems that all business except medicine works on a supply demand ratio in the market. For some reason, they are artificially disallowing this which creates these gaping unfixable problems.
I think you make a ton of valid points here. The way that I look at a tool like this is that we can’t effectively move forward without accurately knowing where we are now. Physicians are underpaid. But if we dont know what the baseline is, it is very difficult to work for more or fair compensation. Without knowing our perceived (and undervalued) value, we are grasping in the dark on an individual doctor level. Then we think what we received is “normal.” This data gives us the leverage to better negotiate as a whole group!
I agree Amy! Where do they get these numbers? I have alot of friends who are dermatologists and they don’t make those salaries! If they join an independent practice they will be paid $250,000./ year! If they work for an equity partner, they will make more the first year but after the 2 year contract they will be put on a percentage of what they bring into the practice! In our area it is saturated with dermatologists & their numbers are low! The family doctors make more than they do unless a dermatologist does aesthetics! However, the midlevels are taking over aesthetics!
Reportedly Medicare pays HMOs 130% of what they allocate for regular Medicare patient care. Medicare pays an extra 40% per visit to Hospitals for their Medicare patients that are seen by their salaried staff, also termed facility fee. The private physicians who see patients in their office are deliberately underpaid and they are the ones struggling the greatest with overhead. Medicare has been reducing physician pay 3% per year for 5 years while inflation during this time has increased 20-25%.
While doctors are getting cut hospitals get an automatic cost of living increase every year.
Doctors don’t support each other and we wouldn’t even dare to spend a few hours in a picket line but nurses have no problem doing so. There is no physician leadership or guidance or resources for us to go to and get help and the insurance companies and government know this. Hence they will keep pushing our buttons
Solution: We are unable to do this on our own.
We need help. The AMA is worthless plus we don’t support it with our dues. You can’t go on strike because too many doctors will continue working to get extra money while the others take time to strike yet they will reap from the benefits that those that bothered to strike achieve.
Sorry for this grim analysis but we are too disorganized to do anything.
Only solutions are:
Join an HMO or hospital HMO
Resign from insurance companies and set your own fee…..good luck
Go concierge….. good luck again
Grin and bear it
Unionize
What is sad is the excellent care that my colleagues and I gave over the years and hoped for as we got older for ourselves, we will not see.
The economics of medicine has destroyed our profession and sustenance.
If/when we ever achieve “universal” healthcare, we’ll fully become what many other countries already are: a 2-tier healthcare system. Tier 1: everyone waiting in long lines to see doctors. Plan ahead +1 year for non-emergent care. As great of an idea healthcare for all is, quality healthcare is a limited resource even for the most developed countries. Tier 2: for those that can afford to do so, pay out-of-pocket for expedited care. Aka concierge. Every single physician I know who has gone concierge: wow, wish I had done that sooner. Didn’t believe it was possible. Feasibility of concierge obviously is different across specialties, demographics of your local region, etc. Doctors collectively bargaining directly with CMS and cutting out HMOs? Great idea, but rounding up all those doctors with all their different interests and practice scenarios…how to make all members feel like their interests are being equally addressed?
This article seems more like an add for Marit than a real addressing of the issue. I find the comments more interesting than the article. I also wonder if the credibility of this site will be questioned and therefore also its value. We could all just post higher salaries than we earn in reality to boost its numbers.
I agree with most comments, especially about the need to organize and the worthlessness of the AMA. How has the AMA allowed a Medicare salary decline in an inflationary environment? It’s pathetic, especially since I do pay my dues.
I also don’t understand why an inflation adjustment is not baked into all physician contracts. I mean, I do understand why, but I think that we should organize to get this in every contract.
I want to add that one of the reasons this happens is because our professionalism towards patient care and wellbeing is exploited. When it is dangerous to the public that a profession strikes, there should be legislation to protect that profession. For instance, our salaries could be adjusted, within a range, to other professions that require similar training and responsibilities, such as lawyers, and, why not? To CEOs pays.
In an ideal world, I propose salaries should vary according to 5 criteria:
– training length and difficulty
– Capacity or skills required (in the case of our profession it requires qualities not everyone has: intelligence, dedication, perseverance)
– Danger (believe it or not ours is up there in terms of danger; thanks, pandemic, for the reminder)
– Responsibility (like an error can cost someone’s life)
– Work demands, such as the need to work long hours, weekends and nights, standing long hours, etc.
Can you think of any profession that scores higher than ours in these five points?
Finally, I was appalled by a fairly recent article in the The Economist titled, “Why doctors in America earn so much”. I intended to respond to this self contradictory article that posited that doctors earn too much and then said the difficulties in the career such as burnout are leading to a decline in physicians. Of course, I was so busy with call that when I got to it, the time for responses had passed. Opinions such as these are damaging to our cause and the fact that physicians are payed even worse in other countries does not help us. The public’s perception of our “lavish”life also does not help.
Amy makes a point which is surprisingly rarely touched upon in physician salary commentary: why is there such a big difference in pay between the different specialties. Why does an ophthalmologist earn 10 times the salary of pediatrician. Again, I know why; the question is why we allow it. The answer about additional training is only partially valid. We could modify our training programs to reduce training time of specialists (like neurologists who only do one internship year).
And finally, is anybody else worried about what AI will do to our salaries? We should be ahead of the changes that are coming and strengthen our lobbying as a group.
I appreciate your comments and can sense your frustration which is shared among all of us physicians. In response to a few of your thoughts:
– I do fully back this endeavor and think it can only help all doctors
– Yes, we all could lie. But how would that help any of us?
– As doctors we make way more than the average American. However we bring a very high value on an individual and societal basis. In my opinion this is what needs to be the focus of any rebuttals.
– The specialty pay gap is not necessarily fair but a reflection of payment structures currently in place. Those will take time to adjust. However the intra-specialty pay gap is much greater and than is what individual physicians should focus on optimizing in my opinion
Appreciate the thoughtful critique. The frustration around pay, lack of inflation adjustments, and the imbalance across specialties is real and a lot of it comes down to how corporatized medicine has become. The public sees the paycheck, but not the years of training or what the day-to-day actually looks like.
One thing I do think we can work on right away is transparency. And try to influence the things we can immediately. I love Jordan’s comment above on intra-specialty pay gap and there is a ton of variation even among people doing similar work. Changing pay gaps across specialties is hard, but within-specialty transparency feels like a place we can start. We actually posted a study on this recently too.
https://www.marithealth.com/posts/when-it-comes-to-pay-the-biggest-variances-are-within-your-specialty
I understand where you are coming from when it comes to not disrupting the status quo in medicine, however, not advocating for revolutionary changes in healthcare financing and reducing pay inequality between primary care physicians and surgeons is a disservice to both taxpayers and the public. By not disrupting the status quo, it tells me that you are part of the problem and not part of the solution. Have you traveled abroad before to understand different countries finance their healthcare systems without so much red tape and over-commercialization of healthcare? Also, physicians and surgeons are part of a union.
Pay transparency is not enough because corporate administrators can inflate physicians salaries by not publishing the updated information due to pay disparities between primary care physicians, medical specialists, and surgeons. Also, older groups of healthcare professionals are the problem and not the solution to the problem. The problem is radical because healthcare policies were implemented to prevent physicians, medical specialists, and surgeons from practicing good medicine and treating their patients in the past 50 years. In other words, big corporations took over non-profit institutions, private practices, and safety-net hospitals.
Very interesting concept ! I am a 61 y/0 Diagnostic Radiologist ( 28 years in practice )and currently scaling back work hours . Teleradiology has allowed me to do this! However the pressure to constantly increase RVU workload is ridiculous! When I work the ER, ordering is out of control with complex exams that should be done on an outpatient basis ( 1 CAT scan can have over a thousand images ). Burn out is immense , it is no longer enjoyable ! It is unrealistic to read a CT brain , facial bones , C spine , chest abdomen and pelvis in 10-15 minutes , with the ED constantly calling for results ! Risk of missing pathology dramatically increases with this model ! We have become the “physical exam “ for everyone in the ED The work loads are unsustainable ! When I look back at my attendings in Residency and their workload then , compared to today , in relation to their income , It is apalling ! No wonder physicians continue to quit medicine ! No other business allows 3rd party middle men to set prices and services between the business and customers ! Hospitals, and Insurance industry along with Medical-Legal has conspired against us ( I don’t give a damn about a” VIP” study anymore either for administrators ! Get in line )The AMA is worthless ! Unfortunately, people will have to be hurt by extenders and unqualified health care workers and public outcry for change will have to occur before anything is done ! The public perception of the healthcare system and physicians in general doesn’t help either ! They dislike us ! We make too much and they pay ridiculous insurance premiums and fees to a corrupt system ! They have been brainwashed into believing healthcare is a constitutional right ! And there better be no mistakes or poor outcomes ! Physicians have become the proverbial whipping boy for corrupt corporate and government control ! Lets face it ! We work in a Fascist system ! Government control of Private industry ! We practice McDonalds drive through healthcare at a Berns Steak house price ! Who’s getting rich ? Administrators , Big Pharma, med manufacturers, drug reps , insurance industry, malpractice lawyers, congress , everyone accept the people actually delivering healthcare ! Our workload and liability risk continues to increase with little to no commensurate increase in income ! Counting the days to retirement , with no regrets ! Sad , a once illustrious profession ruined by Government and corporations !
Excellent comment
The insurance industry has been wrapping coils around our profession since the 1980’s. Prior to this they have influenced lawmakers since the 19th century.
This is great data, but I’m failing to see how such efforts will move the needle unless a crisis develops. Such has always been the case with physician compensation with rare exceptions. Once large numbers of vacancies occur via attrition or physicians simply opting not to enter certain fields in training, then enough pressure develops to enforce change. The clearest example of this phenomenon is call stipends. In many markets, stipends are necessary to attract any physicians. Long gone are the days of claims that it is our duty to take call gratis. Furthermore, any program that seeks to calculate adequate compensation for physicians must also take into account opportunity cost: med school debt, residency indentured servitude, fellowship sacrifice – all leading to earning years lost and massive debt for most of us. It takes decades for physicians to catch up. With the above all taken into consideration, physicians are among the most grossly undercompensated professionals in existence. Frankly, I’m amazed there are enough altruists out there to continue entering medicine. Yes, none of us did it for the money, but there is nothing wrong with expecting fair and appropriate compensation, particularly in the face of exploding C-suite costs across the nation. As for pay gaps, keep in mind hours invested and hours worked along with liability exposure and mental stress that are not neutral factors between specialties. Pay fixing or pay equalization by administrative, legislative, or bureaucratic means will create a medicine much worse than the disease.
Some of the specialty pay gaps have to do with surgical (incl ophthalmology and ENT). vs non surgical specialties Some also has to do w acute call requirements and acute call volumes (Neuro, Cardio, OBGYN) in addition to clinic work …. I do think primary care, internists and pediatricians (incl and perhaps especially peds subspecialists given their longer training and delayed income) are significantly underpaid but we do have to consider some of the variables contributing to the gaps.
These numbers make me so depressed: as an internist/hospice and palliative care doc, my salary has always been much lower than anything listed here.
This is great. However, you can’t simply include “pediatrics” as one specialty. It breaks into almost as many subspecialties as adult medicine, with vastly different pay across each, just as in adult medicine. Would be helpful if articles such as these broke down pediatrics by field. This would help bring light to pediatric subspecialty salary being lower than general pediatrics, which is a real concern.
Pay transparency is not enough because corporate administrators can inflate physicians salaries by not publishing the updated information due to pay disparities between primary care physicians, medical specialists, and surgeons. Also, older groups of healthcare professionals are the problem and not the solution to the problem. The problem is radical because healthcare policies were implemented to prevent physicians, medical specialists, and surgeons from practicing good medicine and treating their patients in the past 50 years. In other words, big corporations took over non-profit institutions, private practices, and safety-net hospitals.