Choosing a specialty is one of the most stressful decisions in medical training.
I remember how heavy that decision can feel. In medical school, it can seem like you are choosing your future identity, income, schedule, training path, and even how other doctors will perceive you.
And of course, compensation enters the conversation. As doctors, we delay income for a long time. Many of us graduate with enormous debt while friends outside medicine are already earning, saving, and building wealth.
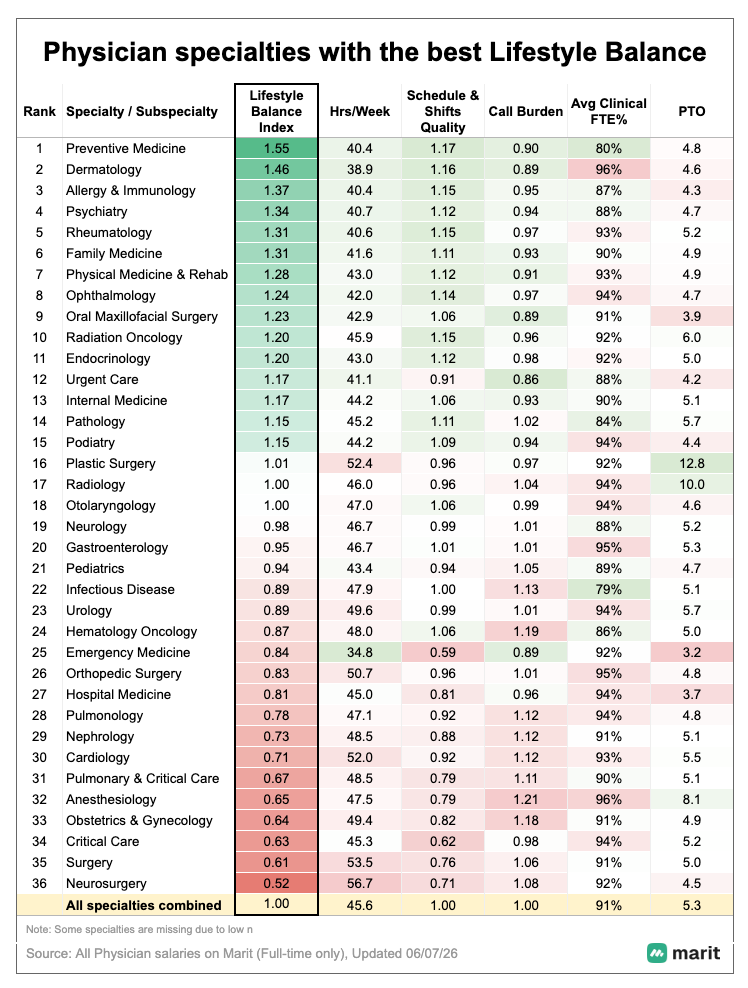
But salary is not everything. That is why this Lifestyle Balance Index, built using Marit compensation and schedule data, is interesting. Instead of looking only at annual compensation, it also accounts for hours worked, call burden, weekday versus weekend work, day shifts, shorter shifts, clinical load, PTO, and schedule quality.
Specialty compensation is not random. It reflects training, expertise, procedural intensity, scarcity, patient acuity, risk, and the economics of the healthcare system. But it also often reflects lifestyle tradeoffs. Higher compensation may come with longer hours, more call, less predictable schedules, and greater physical or emotional intensity.
That does not make one specialty better than another. It just means every specialty has a cost structure, and not all of it is financial.

• Marit has one of the largest anonymized datasets of real physician compensation.
• Verified physicians get a customized MGMA snapshot for their specialty.
• See how compensation changes by specialty, schedule, practice type, and job structure.
• All you do is share your anonymous salary to unlock it.
For survey context, Marit analyzed tens of thousands of anonymous full-time salary submissions from verified clinicians and calculated a Lifestyle Balance Index by specialty. The Index includes several factors that make up the rankings: average weekly hours, schedule quality, call burden, percent clinicial time, average weekly PTO. The factors are normalized (so the average is 1.0) and then combined to create the Index. For full methodology, reach out to [email protected].
High Income Often Comes With Hidden Tradeoffs
When doctors compare specialties, annual income is the easiest number to focus on. It is clean, measurable, and motivating.
But annual income can hide the lived experience.
Some highly compensated specialties in the dataset also involve longer work weeks, more call, more procedures, more emergencies, or less predictable schedules. A physician taking care of high acuity problems at odd hours or carrying call responsibility is often being compensated not just for skill, but also for availability and intensity.
The money often reflects the demands of the work. A surgeon called in overnight is living a different daily experience than a physician whose work is mostly scheduled in advance.
So the better question for students deciding their specialty is not simply, “How much does this specialty pay?” A better question is, “What might this specialty require of me to earn that pay?”
Predictability Is a Form of Wealth
The opposite pattern matters too.
Some specialties with lower average annual compensation show more favorable lifestyle characteristics. Fields like allergy and immunology, rheumatology, psychiatry, family medicine, preventive medicine, PM&R, and ophthalmology generally show more predictable schedules, more weekday work, more day shifts, and fewer lifestyle disruptions compared with many higher intensity fields.
Again, this does not mean these specialties are easy. Every field has hard parts. Primary care doctors deal with inbox burden and administrative friction. Psychiatrists manage some of the hardest human suffering imaginable. Rheumatologists and allergists care for chronic disease that requires patience and nuance.
But the structure of the work can be different. And structure matters.
A doctor making less on paper but working a more predictable schedule may have more energy to be present at home, exercise, build a side gig, invest consistently, or avoid the kind of burnout that forces an early exit from medicine.
The point is not that one specialty is more virtuous than another. The point is that some specialties may make it easier to build a life with more control, and that can be priceless.
The Outliers Are the Most Interesting Part
The most interesting part of this data is not the obvious tradeoffs. It is the exceptions.
Dermatology is the classic example. In this dataset, it combines high compensation with favorable schedule characteristics, including a high percentage of weekday work, day shifts, and shorter shifts. The appeal is not just income. It is the combination of income, predictability, and practice optionality.
Radiation oncology is another interesting example. It shows strong compensation with a relatively favorable schedule profile. The work is specialized and technologically complex, but the care model may allow for more scheduled work than fields driven heavily by emergencies and call.
Ophthalmology can also offer a strong blend of pay, procedural work, and schedule predictability.
Emergency medicine is a different kind of outlier. The weekly hours are lower than many other fields. But the work is often nights, weekends, holidays, and rotating shifts. Thirty five hours per week can feel very different depending on when those hours occur.
Lifestyle is not one variable. Hours matter. But so do nights, weekends, call, acuity, inbox burden, patient volume, autonomy, and emotional intensity.
• Marit has one of the largest anonymized datasets of real physician compensation.
• Verified physicians get a customized MGMA snapshot for their specialty.
• See how compensation changes by specialty, schedule, practice type, and job structure.
• All you do is share your anonymous salary to unlock it.
The Average Does Not Tell the Whole Story
This is where lifestyle balance meets compensation variance.
In a previous piece, “Two Doctors. Same Specialty. $500K Apart. Why?” I wrote about one of the biggest misconceptions doctors carry, and it is one I carried early in my career. I assumed specialty choice determined earning potential.
Specialty choice matters. But the biggest pay gap in medicine is often not between specialties. It is inside them.
Two doctors with the same board certification can be separated by hundreds of thousands of dollars a year. The reason is rarely just effort or talent. More often, it is job structure.
One physician may be employed on a fixed salary with a modest bonus. Another may have productivity upside, partnership, ASC distributions, ancillary revenue, or ownership. One may earn more by taking more call, nights, or weekends. Another may earn more because the economics of the practice are better aligned.
This matters for lifestyle. In high variance specialties, there may be more opportunity to shape income through ownership, payer mix, procedural volume, call structure, or geography. But there may also be more temptation to chase income by simply working more. In lower variance specialties, compensation may be more standardized, so schedule choices may become the bigger lever.
That is why averages can mislead us. An average salary tells you what a specialty looks like in the middle. It does not tell you what the range looks like, or what tradeoffs create that range.
Specialty Is Not Destiny
One reason this topic is sensitive is that doctors are deeply tied to their specialties.
We introduce ourselves by specialty. Hospitals organize us by specialty. Patients identify us by specialty. Other doctors make assumptions about us based on specialty. Over time, a specialty can become a core part of how we see ourselves.
That is why conversations about compensation and lifestyle can feel personal. Nobody wants to hear that their field has a “bad lifestyle” or that another field has it easier. Those statements are too simplistic anyway. Every specialty has hard parts.
The better way to think about this is not judgment. It is tradeoffs. Each field has a different blend of intellectual demands, procedural demands, emotional demands, training length, compensation, autonomy, and schedule structure.
And within the same specialty, two doctors can have completely different lives. One may be employed by a hospital system with heavy call and limited autonomy. Another may be in a well structured private practice with ownership and more control. Another may work part time, do locums, focus on academics, build a niche practice, or create nonclinical income streams.
A specialty does not mean you are locked into a one-size-fits-all life.
That is why financial education is so important for physicians. The more financially secure you are, the more flexibility you have to shape your practice. You can negotiate from a position of strength. You can say no to a bad job. You can reduce clinical time if needed. You can choose a slightly lower paying role that gives you a healthier life.
Financial independence does not remove every hard part of medicine. But it gives you options. And options are often the real measure of wealth.
• Marit has one of the largest anonymized datasets of real physician compensation.
• Verified physicians get a customized MGMA snapshot for their specialty.
• See how compensation changes by specialty, schedule, practice type, and job structure.
• All you do is share your anonymous salary to unlock it.
The Takeaway
The Lifestyle Balance Index is not useful because it tells us which specialty is superior. That is the wrong way to read it.
It is useful because it reminds us that compensation has context.
Higher paying specialties often pay more for real reasons: training, skill, risk, scarcity, procedural intensity, and the burden of being available when patients need you. But they may also involve lifestyle tradeoffs that do not show up in a salary survey.
At the same time, specialties with more favorable lifestyle profiles may offer forms of wealth that are harder to measure: predictability, energy, longevity, time with family, and the ability to enjoy the money you earn.
For students and residents, the lesson is to look beyond salary and prestige. Ask what the attending life really looks like: call, weekends, ownership, autonomy, and what people wish they had known.
For attendings, the lesson is empowering. You may not be able to change your specialty, but you can often change your structure. You can build margin, reduce debt, invest, pursue ownership, and create options.
And sometimes, that is the real path to a better physician life. Not choosing the perfect specialty, but building enough control that your specialty does not completely control you.
What do you think? Does your specialty’s compensation and lifestyle tradeoff match your lived experience? Let me know in the comments below!











